Air Purification in an Oral Surgery setting
I have investigated some of the air purification systems around and I am delighted to announce that I am the first dental/oral surgery practice in Ireland to have acquired the Novaerus air purifications system in our practice at Castle Clinic Dalkey. I have acquired the defender 1050 for the surgery and the N/V 800 for the waiting room and recovery room. The air purification machines run continually and whilst the manufacturer is not claiming that they sterilise a room, as it is not a closed environment, they do claim they significantly reduce the bio-burden at any moment and are effective for coronavirus. The larger unit, the defender 1050, that we placed in the surgery causes a x4.14 Net Log reduction in 15 minutes of bio-burden when tested using the MS2 bacteriophage. This bacteriophage MS2 is considered a surrogate for Covid-19 given its RNA genome and size. The only difference I could see is that the surrogate virus is not enveloped and Covid is.
Please click on the link ‘Efficacy of Novaerus NV 1050 device against Aerosolised MS2 Virus’ to read the paper by Balarahti and Trolinger’.
The mechanism with Novaerus air purification products centre around plasma technology using the dielectric charge barrier that distorts/decays the bacteria and viral membrane to such an extent that they leak their intracellular contents and are killed. The defender 1050 has in addition a built in PRE-FILTER and HEPA FILTER in addition to a CARBON filter. The N/V 800 does not have the filters and uses the plasma technology only and is smaller. We have positioned this in the waiting room to mitigate against viral airborne transmission with aerosol that can travel considerable distance and possibly stay viable for hours within a building.
Air purification products such as stand alone HEPA filters were marketed recently over one year ago in the U.K. through the BDA for use when removing amalgam restorations, removing bacterial and particulate matter aimed at eliminating the risk to all when working in the Mercury cloud. The I-Q Air, a Swiss product, has a stand alone unit and a unit that has a flume like an elephants trunk that is positioned as close to the working area as is possible. The HEPA filter does not kill bacteria or viruses it simply collects them and as a result there is colonisation in the filters. The HEPA filter is not effective in trapping virus as they are too small. The Irish distributor when I contacted him, claimed it would be useful for coronavirus, he could provide no data on the product he was distributing for virus elimination. There was a significant price differential between the U.K distributor and the Irish distributor for the I-Q Air. I would not recommend this product to Irish dentists to tackle airborne transmission of coronavirus in a dental surgery setting. It appears ineffective and I could find no data to support its use with regards to viral airborne bio-burden control.
The next air purification trapping system mechanism is called Electrostatic Precipitation and uses a combination of ionisation with filtration.The technology produces an electrical current, giving pathogens in the air either a positive or negative charge before they are passed through an electrostatic filter with the opposite charge.
‘Electrostatic Precipitation can trap smaller particles in the air however the technology encounters problems with larger particulate (bacteria, pollens,acrylic etc).
The weight of larger particles combined with the airflow forces the particles to overcome the attraction that the electrical field creates, allowing them to stick to anything in the room that is carrying an electrical charge, such as surfaces and people
So in an oral surgery or dental surgery environment this super sticky bio-burden that is created renders the product unsuitable. There is an Irish dental distributor marketing such a product at present for use in the surgery.
Another trapping mechanism is ‘Ionisation using electrical power to create positive and negative ions in the air. These ions attract airborne pathogens, attach themselves to them and fall to the floor or other available surfaces.
Ionisation in a healthcare setting has some limitations:
- The particulate, newly attached to the ions, can land on walls, curtains, tables, beds&patients.
- This technology can interfere with wound healing
So in summary none of the trapping air purification systems seem suitable for oral surgery / dental surgery environments.
This moves us onto exploring the ‘killing technologies’…the first is Ultraviolet light.
UVGI is electromagnetic radiation that can destroy the ability of microorganisms to reproduce by causing photochemical changes in nucleic acids.
While UVGI can be an effective method of cleaning the air, there are some limitations:
-
Exposure time – the exposure time required for the pathogens to be affected can not be realised in real patient environments.
-
Line of sight – bacteria traveling in clusters can promote shadowing; bacteria on the outside of the cluster will protect those on the inside, which cannot be detected by the UVGI source. The bacterial spores can stack on surfaces, making them extremely difficult to destroy.
-
Mutagenic effect – short-term exposure to UVGI has been proven to mutate the structure of bacteria and viruses, making them even more dangerous.
-
High maintenance
-
High operating cost
This does not lend itself to dental surgery oral surgery environments. The final killing method I could find is chemicals such as ozone and hydrogen peroxide, while effective, are primarily point-in-time solutions.These methods cannot be carried out in the presence of humans.
-
During chemical cleaning, typically the space in question is required to be out of commission for a period of time. This allows for room preparation, cleaning and a waiting period until the room is safe for human use again.
-
After chemical cleaning, the sterilized space is instantly subject to airborne contaminants once doors and windows are opened and/or people re-enter the room.
So that leads me onto the di-electric barrier plasma technology with Novaerus. From a safety point of view this product does not produce ozone, it does not produce ionised super sticky particles all over the surgery, it kills virus, it is used currently in Neo-natal units, ITU, theatres and hospitals as per manufacturer. I also note that Wuhan is using the same technology having being endorsed by the Chinese. This product also has some studies. They are limited but so is all of our current information on coronavirus. I get the feeling that some of the dental distributors are getting air purification systems designed primarily for the office and home and then marketing these be placed directly into the dental surgery with no research or understanding of the scope of works of the profession. It is up to the dentist and oral surgeon to research all products and establish that they are safe in a surgery environment and CE approved. I wonder if these technologies as introduced by manufacturers and distributors in Ireland into the surgery should have to go through medical device regulations to ensure all technologies are validated and appropriate?
This was my adventure on airborne transmission and coronavirus in the oral surgery / dental surgery practice over the last three weeks that ended with the purchase of the Defender 1050 and N/V 800. We are opening an emergency Oral Surgery Clinic in Dalkey as we now have FFP3, FFP2 masks, face shields, air purification systems, gowns and local protocols in place. We are using the PARA principles (PPE, Avoiding unnecessary activity, Reducing number of people exposed to risk and Abbreviating the procedure by having the most experienced dentist/oral surgeon operate). This all leads to optimising safety for all members of the team from surgeon to receptionist and from patient in the chair to the patient who has yet to attend. Our fallow time is going to be greatly reduced and it gives our team confidence at work and reassures our patients.
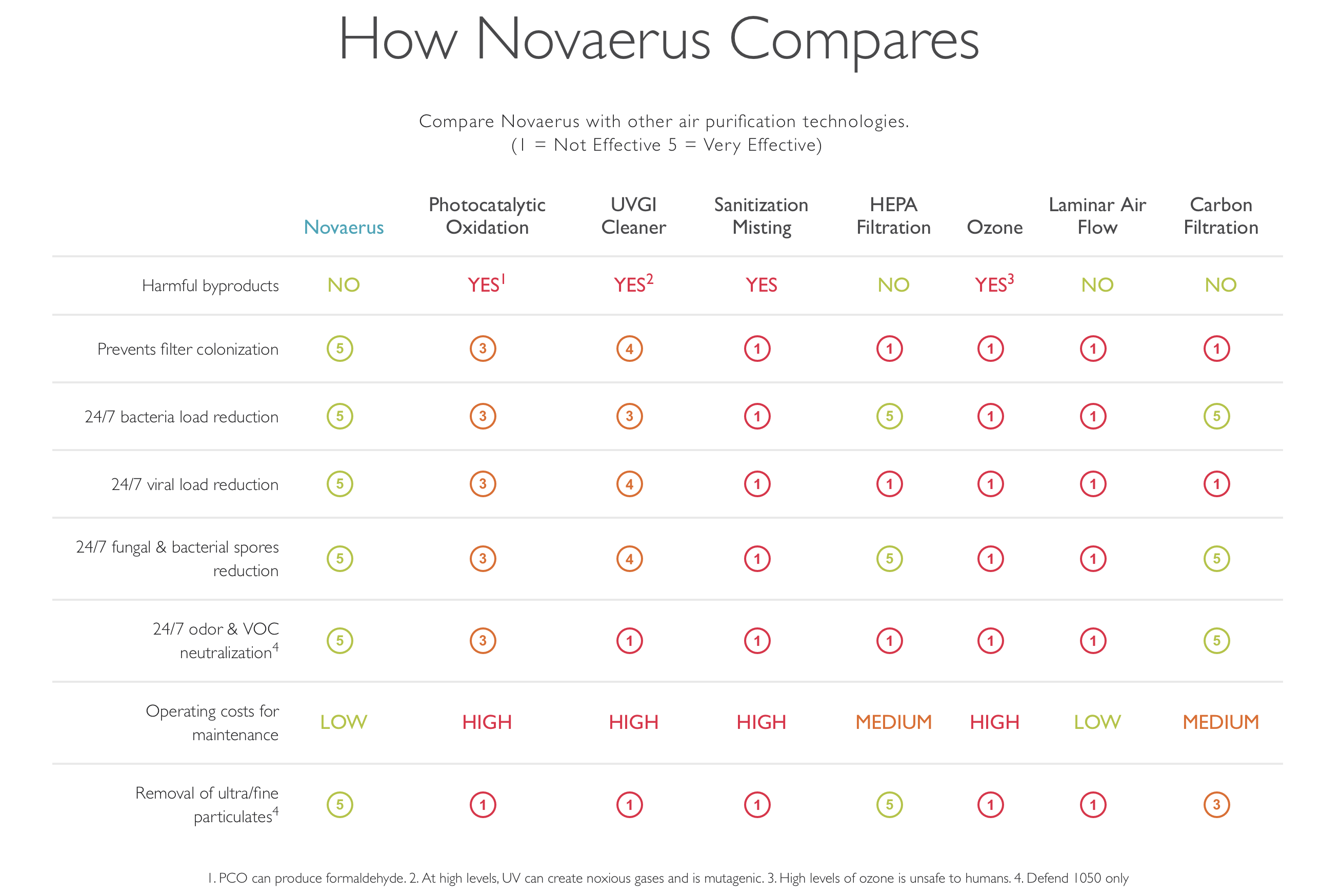
Below is a summary from the manufacturer’s website on the comparison